
Key Takeaways
- Diastasis recti is common postpartum but often overlooked.
- Key signs include doming, core weakness, and persistent belly bulge.
- Avoid high-pressure exercises early; prioritise rehabilitation.
- Early assessment improves recovery outcomes.
Having a baby changes your body. Many new mothers, after birth, notice a rounded tummy that persists after they lose their baby weight. But if the weeks have passed, and if you are noticing a postpartum belly pooch that does not feel or look like yours, with softness around the middle that won’t shift or bulge, it may be diastasis recti, a common postpartum condition that often goes unrecognised.
Here’s what it is, why it happens, and common diastasis recti symptoms to spot.
What Is Diastasis Recti?
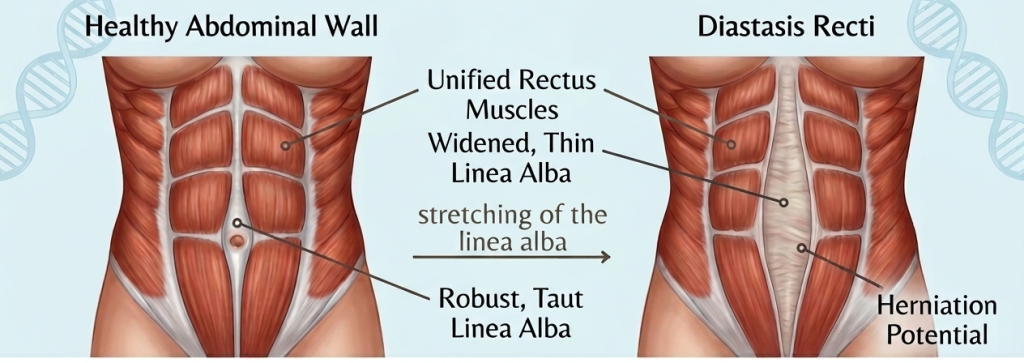
Around one third of women experience postpartum diastasis recti, which is when the two muscles that run down the middle of your stomach separate.
Diastasis recti typically occurs during pregnancy as the uterus expands, as it places increasing pressure on the abdominal wall, making them longer and weaker, before gradually pushing the two muscle groups apart. The result is a gap where there was once a unified, supportive core.
Diastasis recti typically develops in the third trimester and may not be obvious until several weeks after birth. The abdomen may appear pushed outward, creating a pooch that diet and general exercise alone do not resolve.
While many women experience some degree of abdominal separation during pregnancy, for some, the muscles do not naturally return to their original position postpartum. Left unaddressed, it can lead to core instability, lower back pain, poor posture, and even incontinence.
How To Tell If You Have Diastasis Recti
There are several common symptoms of diastasis recti.
Visually, the most recognisable symptom is a bulge or “pooch” above or below the belly button, one that persists even as your pregnancy weight reduces. You might also notice a soft, almost jelly-like feeling around the navel. Another key sign is “coning” or “doming” – a ridge that rises along the midline of your stomach when you engage your core, such as when sitting up, coughing, or lifting your baby.
Diastasis recti can also show up in more subtle, functional ways. Low back pain is a common complaint, often dismissed as a side effect of feeding positions or carrying your baby.
Some women experience a sense of pelvic instability or heaviness, while others find everyday movements, such as getting out of bed, standing up from the sofa, bending down, or lifting, unexpectedly difficult.
How To Check For Diastasis Recti At Home
A simple at-home check can give you a useful starting point before speaking to a GP or physiotherapist.
You can check the size of the separation with this simple finger test:
- Lie on your back with knees bent, feet flat on the floor.
- Place two or three fingertips horizontally across the midline, just above or at the belly button.
- Slowly lift your head as though starting a crunch.
- Feel for a gap between the muscle walls.
- You likely have diastasis recti if space allows you to fit three or more fingers.
Also note whether your fingers sink down rather than meeting firm resistance, as this can indicate reduced tension in the connective tissue.
This quick test can help you tune into what’s happening in your body, but a women’s health physiotherapist will be able to assess more accurately and guide you on what to do next.
Exercises To Avoid With Diastasis Recti
In the early postpartum period, it is generally wise to avoid exercises that create visible doming or coning along the midline. Traditional crunches, sit-ups, reverse crunches, double leg lifts and full planks may place too much load on the abdominal wall before core control has recovered.
High-impact exercise such as running and jumping may also be too demanding too soon, particularly if you notice leaking, heaviness or pelvic floor symptoms.
The main sign that a movement is not right yet is a ridge or bulge forming through the centre of the abdomen. If that happens, the exercise should be modified or paused.
Will Diastasis Recti Resolve on Its Own?
Diastasis recti may improve naturally after birth, but recovery varies from one woman to another.
In milder cases, especially where the separation is small, the body may begin to heal naturally as the connective tissue regains tension. However, larger or more persistent separations often take anywhere from six to twelve months and may require guided rehabilitation.
In some women, the gap doesn’t always fully close on its own, particularly if symptoms like back pain, pelvic floor issues, or visible doming persist.
It’s advisable to seek support or diastasis recti treatment if:
- The gap hasn’t noticeably reduced by six to eight weeks postpartum.
- You are experiencing back pain, pelvic pressure, or leaking.
- Doming or coning persists during everyday movements.
- Core weakness is affecting everyday function.
A women’s health physiotherapist can assess the separation more accurately and advise on the safest next steps.
When Should I Seek Assessment for Diastasis Recti?
Diastasis recti is common and often mistaken for stubborn weight to general post-baby changes. The reassuring part is that it’s treatable.
For best outcomes, it’s recommended to seek assessment and postpartum diastasis recti treatment around 6–8 weeks postpartum, when tissues are still in an active healing phase and typically respond better to intervention. Early recognition puts you in a stronger position to recover well and feel like yourself again.
If any of this sounds familiar, consider booking a postpartum assessment or speaking to a women’s health physiotherapist. At Prologue Wellness, our team will gladly help you with a professional assessment, where we can provide an accurate diagnosis and personalised treatment plan.
References:
- Wu, L., Gu, Y., Gu, Y., Wang, Y., Lu, X., Zhu, C., Lu, Z. and Xu, H. (2021), Diastasis recti abdominis in adult women based on abdominal computed tomography imaging: Prevalence, risk factors and its impact on life. J Clin Nurs, 30: 518-527. https://doi.org/10.1111/jocn.15568

